Disability accumulation can build gradually—so it’s important to continue monitoring it proactively1
Even when RRMS patients appear stable, smoldering neuroinflammation continues to cause damage.1,2
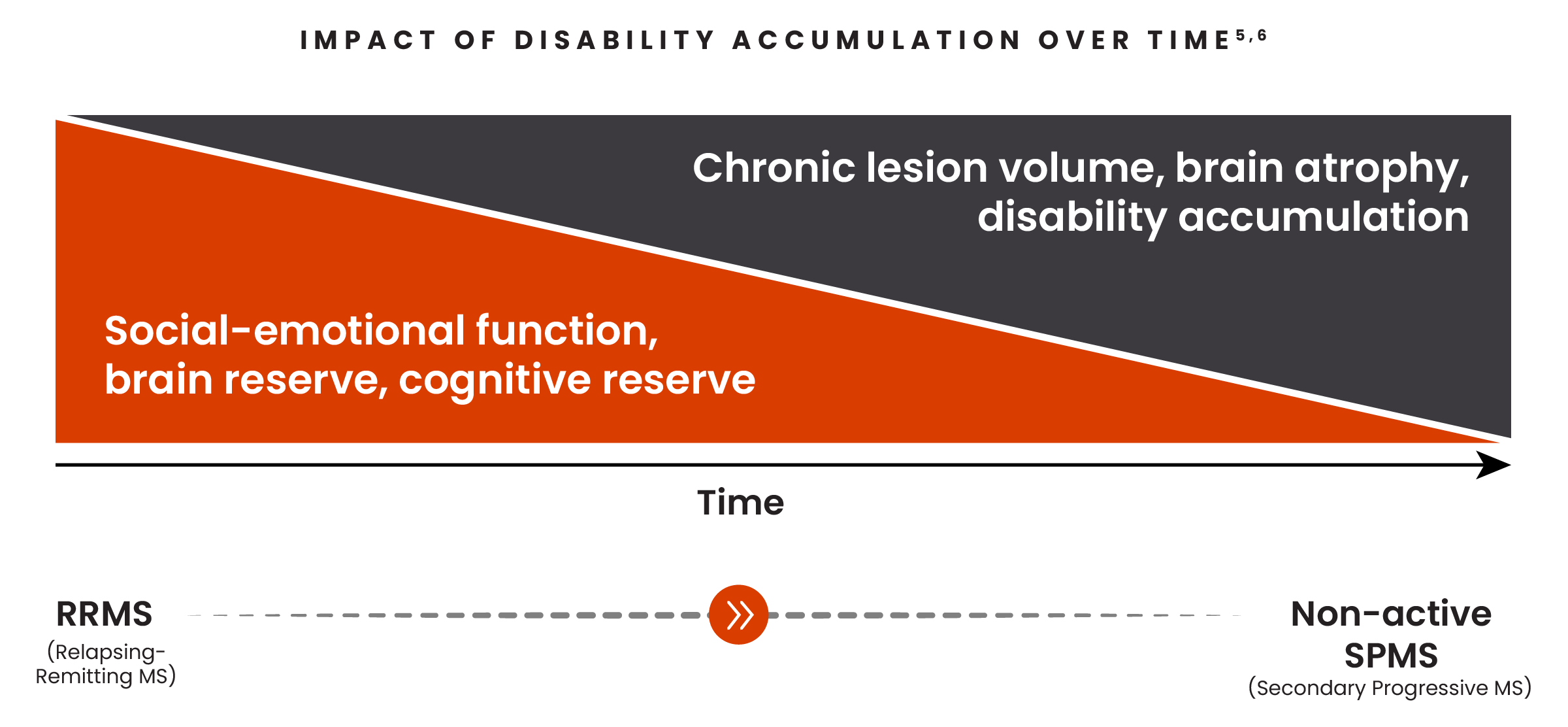
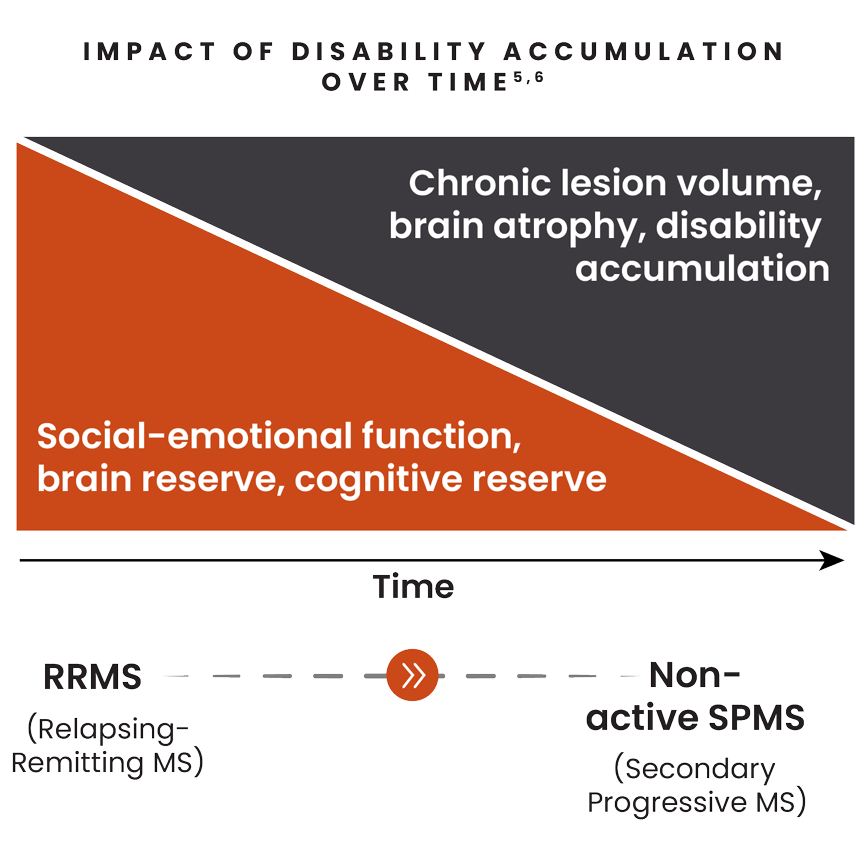
The damage from smoldering neuroinflammation can accumulate slowly and manifest as gradual physical and/or cognitive changes over years prior to naSPMS diagnosis.1,2
Symptoms could be gradually building before revealing themselves as clinically detectable disability accumulation.3,4
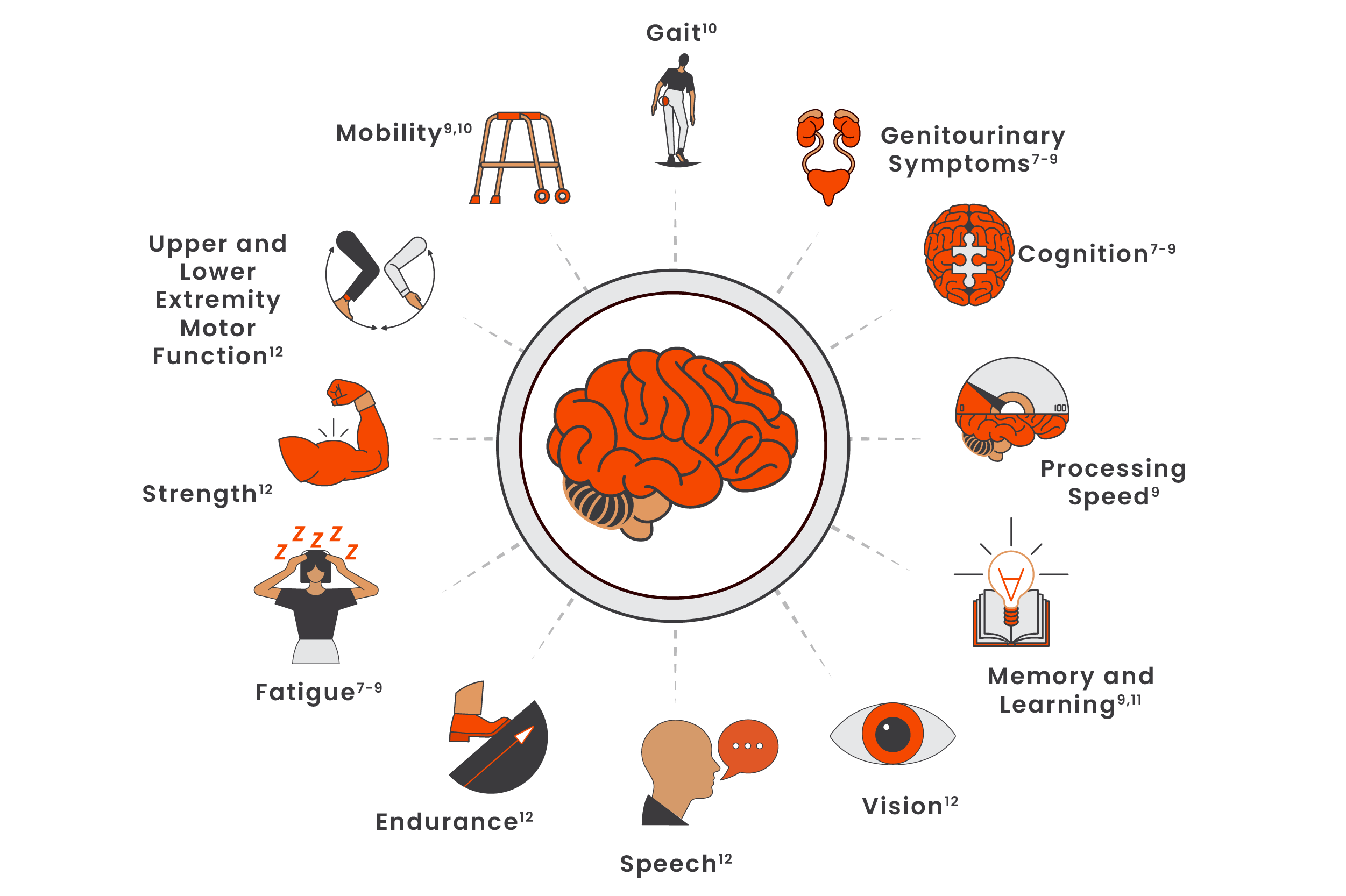
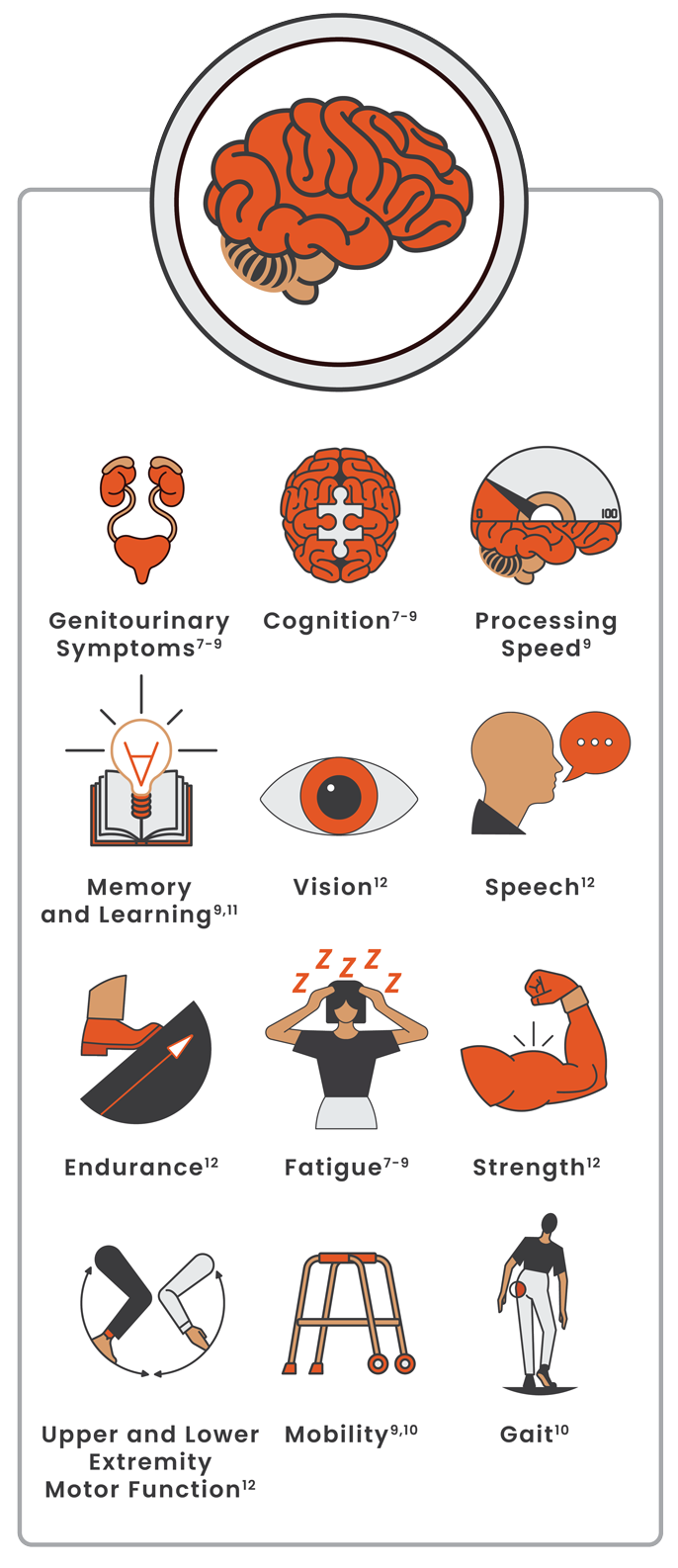
Physical and cognitive changes due to smoldering neuroinflammation may appear early7-9
Worsening fatigue, cognitive deficits, and bowel/bladder symptoms have been reported as early signs of PIRA in RRMS.7-9
While patient reports are an integral part of detecting and acknowledging gradual changes of disability, patients may experience difficulty noticing the gradual onset of symptoms, connecting their disability with their MS diagnosis, and/or articulating their signs and symptoms clearly.9
Concerns your patients may bring to your attention7:
- Having to stop or decrease playing sports such as tennis, running, etc
- Experiencing difficulty doing more than one task at a time
- Reducing social activities
- Being less productive at work or having difficulty doing current work vs previously
Monitoring disability accumulation
Monitoring changes in the signs of disability may include:
- Establishing a baseline assessment, including cognitive testing9
- Assessing and acknowledging patient concerns by proactively asking questions and encouraging open communication9
- Regularly using clinical assessment tools in practice such as the timed 25-ft walk (T25-FW), 9-hole peg test (9-HPT), and Symbol Digit Modalities Test (SDMT)13,14
- Reframing patient conversations by inviting them to compare their current abilities vs a specific life event over longer periods of time (eg, birthday, holiday)7
Managing disability accumulation
Nonpharmacological interventions may help manage a patient’s disability accumulation and may improve quality of life:
It’s important to continue proactively monitoring disability accumulation over the course of MS1
Smoldering Stories
Smoldering neuroinflammation may go unaddressed—hear Sonia's story.

References:
-
Giovannoni G, Popescu V, Wuerfel J, et al. Smouldering multiple sclerosis: the ‘real MS’. Ther Adv Neurol Disord. 2022;15:17562864211066751. doi:10.1177/17562864211066751
-
Katz Sand I, Krieger S, Farrell C, Miller AE. Diagnostic uncertainty during the transition to secondary progressive multiple sclerosis. Mult Scler. 2014;20(12):1654-1657. doi:10.1177/1352458514521517
-
Cree BAC, Hollenbach JA, Bove R, et al; University of California, San Francisco MS-Epic Team. Silent progression in disease activity-free relapsing multiple sclerosis. Ann Neurol. 2019;85(5):653-666.
-
Scalfari A. MS can be considered a primary progressive disease in all cases, but some patients have superimposed relapses - Yes. Mult Scler. 2021;27(7):1002-1004.
-
Inojosa H, Proschmann U, Akgün K, Ziemssen T. A focus on secondary progressive multiple sclerosis (SPMS): challenges in diagnosis and definition. J Neurol. 2021;268(4):1210-1221.
-
Macías Islas MÁ, Ciampi E. Assessment and impact of cognitive impairment in multiple sclerosis: an overview. Biomedicines. 2019;7(1):22. doi:10.3390/biomedicines7010022
-
Bayas A, Schuh K, Christ M. Self-assessment of people with relapsing-remitting and progressive multiple sclerosis towards burden of disease, progression, and treatment utilization results of a large-scale cross-sectional online survey (MS Perspectives). Mult Scler Relat Disord. 2022;68:104166. doi:10.1016/j.msard.2022.104166
-
Portaccio E, Bellinvia A, Fonderico M, et al. Progression is independent of relapse activity in early multiple sclerosis: a real-life cohort study. Brain. 2022;145(8):2796-2805.
-
Lakin L, Davis BE, Binns CC, Currie KM, Rensel MR. Comprehensive approach to management of multiple sclerosis: addressing invisible symptoms—a narrative review. Neurol Ther. 2021;10(1):75-98.
-
Ziemssen T, Derfuss T, de Stefano N, et al. Optimizing treatment success in multiple sclerosis. J Neurol. 2016;263(6):1053-1065.
-
Halper J, Kennedy P, Miller CM, Morgante L, Namey M, Ross AP. Rethinking cognitive function in multiple sclerosis: a nursing perspective. J Neurosci Nurs. 2003;35(2):70-81.
-
Dillenseger A, Weidemann ML, Trentzsch K, et al. Digital biomarkers in multiple sclerosis. Brain Sci. 2021;11(11):1519. doi:10.3390/brainsci11111519
-
Koch MW, Mostert JP, Wolinsky JS, et al. Comparison of the EDSS, timed 25-foot walk, and the 9-hole peg test as clinical trial outcomes in relapsing-remitting multiple sclerosis. Neurology. 2021;97(16):e1560-e1570. doi:10.1212WNL.0000000000012690
-
Brochet B, Deloire MSA, Bonnet M, et al. Should SDMT substitute for PASAT in MSFC? A 5-year longitudinal study. Mult Scler. 2008;14(9):1242-1249. doi:10.1177/1352458508094398
-
Döring A, Pfueller CF, Paul F, Dörr J. Exercise in multiple sclerosis – an integral component of disease management. EPMA J. 2012;3(1):2. doi:10.1007/s13167-011-0136-4
-
Feinstein A, Amato MP, Brichetto G, et al. Study protocol: improving cognition in people with progressive multiple sclerosis: a multi-arm, randomized, blinded, sham-controlled trial of cognitive rehabilitation and aerobic exercise (COGEx). BMC Neurol. 2020;20(1):204. doi:10.1186/s12883-020-01772-7
-
Stampanoni Bassi M, Centonze D. Specific dietary interventions to tackle obesity should be a routine part of recommended MS care – Yes. Mult Scler. 2020;26(13):1627-1629. doi:10.1177/1352458520916701
-
Kheirouri S, Alizadeh M. Dietary inflammatory potential and the risk of neurodegenerative diseases in adults. Epidemiol Rev. 2019;41(1):109-120. doi:10.1093/epirev/mxz005
-
Gil-González I, Martín-Rodríguez A, Conrad R, Pérez-San-Gregorio MÁ. Quality of life in adults with multiple sclerosis: a systematic review. BMJ Open. 2020;10(11):e041249. doi:10.1136/bmjopen-2020-041249
-
Blankespoor RJ, Schellekens MPJ, Vos SH, Speckens AEM, de Jong BA. The effectiveness of mindfulness-based stress reduction on psychological distress and cognitive functioning in patients with multiple sclerosis: a pilot study. Mindfulness. 2017;8(5):1251-1258. doi:10.1007/s12671-017-0701-6